Developing Children’s Burn Treatment Programs in Developing Countries
Introduction:
Burns are one of the most neglected areas of health care in developing countries. These countries have 90% of global burn injuries, with 70% of these injuries occurring in children. While there have been major improvements in burn care in high-income countries, making it quite possible for patients with burns of more than 90% of body surface area to survive, in countries such as Pakistan, burns of over 40% are frequently fatal, there are only 8 specialized burns units for a population of 182 million people (WHO) [1 BOX 4-5]. Even minor burns can lead to significant illness and permanent disability as a lack of hospital services, expensive care, recurrent wound infections, delayed wound healing and the formation of contractures (NATION) [2].
Method:
In spite of four medical mission trips per year for 9 years the waiting list of burn patients increased by 60% yearly. This establishes the basis for a permanent pediatric burn unit in partner hospital in South East Asia region of our global community. After allocation of area to establish the permanent center next step was to charter the team, furnished and equipped the unit, create the guidelines, educate staff on the principles of burn care and launch the fundraising.
The Burn Unit present firm commitment to Pediatric burn patients by developing:
- Infrastructure for 12 bedded facility with complete protocols and regulation
- Surgery three days a week, average of 600-700 surgeries yearly
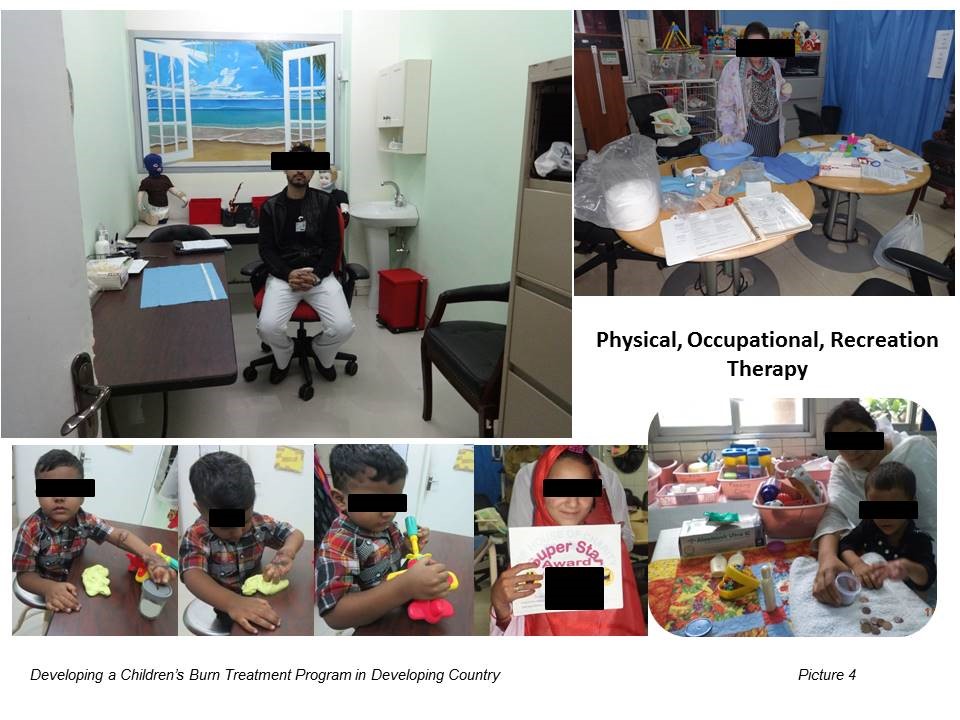
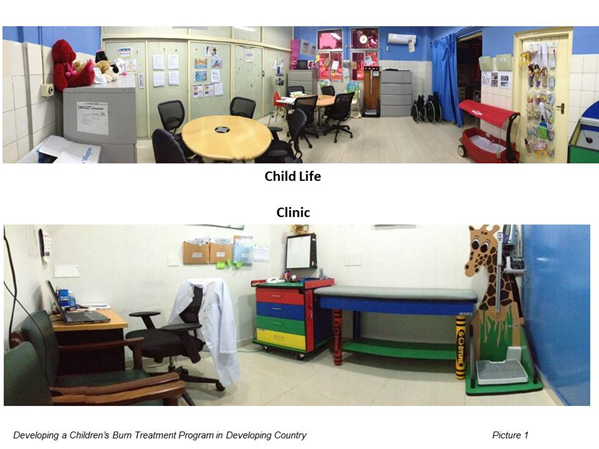
- Medical photography, medical record keeping, child life, counseling, outpatient and day surgery (minor burns)
- Physical, occupational and recreational therapy, splinting, pressure garment and scar message;
- Research data collection;
- Design to run prevention/safety campaigns
- Education and training of health professionals with technology transfer from USA & other countries
The main goal is not only save lives but prevent deformity and ensure that they become useful member of the society.
Result
Four indicators were used to determine the result: Length of stay, readmission, infection and patient satisfaction (3) survey (1400 patients in 2013-2015).
Meeting four quality indicators shows that for 1400 patients, the program was safe and effective and pilot project has met all its above goals. Services provided without regard to race, color, creed, sex or sect, disability, or ability of a patient or families to pay
Conclusions:
With the success of pilot program the management and team are expanding the pediatric burn program into Children’s Burn Center.
Applicability of Research to Practice
Research has improved the quality of burn care. Like nursing staff were unfamiliar that how rehab will reduce the disability among children with burn injuries, the survey forms will improve quality of care and prevention will reduce burn injuries.